
Research done by Dr. Henriette C. Jodal and co-workers from the Clinical Effectiveness Research Group at the University of Oslo and Oslo University Hospital, shows that interval cancers after a negative colorectal cancer screening test do not have a worse prognosis as compared to clinically detected cancers.
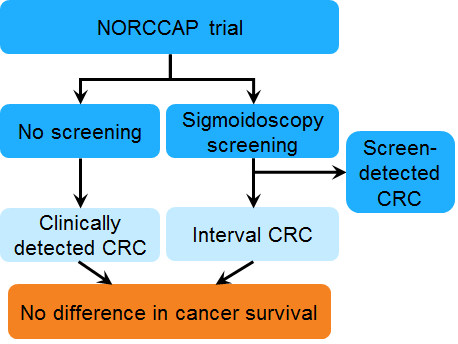
The group took advantage of a randomised controlled sigmoidoscopy screening trial, the Norwegian Colorectal Cancer Prevention (NORCCAP) trial, and compared colorectal cancer-specific and all-cause mortality of individuals with interval colorectal cancer to individuals diagnosed with colorectal cancer in the non-screened control group.
Management of interval cancers
Sigmoidoscopy screening has been shown to reduce colorectal cancer incidence and mortality , and screening has been introduced in many countries. While FOBT (fecal occult blood test) screening is offered every year or every second year, sigmoidoscopy screening is offered with longer time intervals between screening examinations (every 5 to 10 years or longer). Thus, the issue of interval cancer may be of greater importance. There is limited knowledge on the prognosis of interval cancer after sigmoidoscopy screening. As colorectal cancer screening becomes more widespread, optimal management of interval cancers will become an issue of increasing importance. Indeed, if they are more lethal than colorectal cancers in general, a more aggressive initial treatment might be justified, but the evidence for this is currently lacking.
Interval cancer: Cancer occurring after screening.
Endoscopy: a flexible tube with a camera used to investigate your GI-tractus.
Sigmoidoscopy: endoscopic procedure including distal part of colon.
Few studies done
The concept of interval cancers is well known, but scarcely studied scientifically. Most studies on the prognosis of interval cancers concern breast cancer, and many are hampered by lack of a valid control group or short follow-up time. Only a few existing studies on interval cancers apply a non-screened, age-matched population from the same time-period with sufficiently long follow-up. These studies are limited to breast cancer screening, prostate cancer screening, and FOBT screening. A recent review of the evidence from molecular biology and from human studies of different cancer types, found no evidence supporting the theory that interval cancers are more lethal.
Challenging beliefs
As colorectal cancer screening becomes more widespread, optimal management of interval cancers will become an issue of increasing importance. Jodal’s study shows that both colorectal cancer-specific and all-cause mortality of interval cancer after a normal sigmoidoscopy screen are similar to that of a clinically detected cancer in a non-screened control group.
The Clinical Effectivenes Research Group’s findings challenge the belief that rapidly growing interval cancers are more lethal than clinically detected cancers.